Source: www.onclive.com
Author: Silas Inman
The frontline treatment for patients with head and neck cancer is largely dominated by surgery and radiation therapy, with ongoing efforts to find biomarkers and other strategies to better individualize care. The leading markers used to tailor therapy are human papillomavirus (HPV) status, which typically signals the aggressiveness of the disease, and PD-L1 expression level, which may help guide selection of immune checkpoint inhibitor (ICI) therapy.
These markers are gaining notice in different settings. HPV status has broad applicability across head and neck cancers, whereas the clinical utility of PD-L1 expression remains a more nuanced question.
HPV-Positive Tumors
Approximately 70% of head and neck cancers, specifically oropharyngeal cancers, are positive for HPV, with most cases associated with the HPV-16 subtype. These tumors appear most commonly in nonsmoking White men with a mean age of diagnosis of 60.3 years (SD, 10.8) for oropharyngeal cancer and 63.2 years (SD, 12.7) for other types of head and neck cancers.1,2
Moreover, HPV-positive tumors typically fall into a low- to intermediate-risk category, with 5-year overall survival (OS) outcomes far superior compared with rates for HPV-negative tumors, which are typically caused by smoking. For patients with HPV-associated head and neck cancers, the 5-year OS rate ranges from 75% to 80% compared with 45% to 50% for those with HPV-negative tumors.3
In many cases, although the prognosis is more favorable for patients with HPV-positive tumors, the treatment is the same as it is for HPV-negative tumors. However, with the introduction of ICIs and other options, deintensified treatment regimens are being explored for patients with head and neck cancer, based on their HPV status coupled with clinical characteristics.
“We really want to cure these patients. These are young patients who are otherwise healthy who have decades of life. Even an incremental decrease in the outcome of survival is a concern, but we’re balancing that with the toxicity of the therapies,” Glenn J. Hanna, MD, said during a presentation at the 40th Annual CFS®: Innovative Cancer Therapy for Tomorrow in November 2022. He is director of the Center for Salivary and Rare Head and Neck Cancers at Dana-Farber Cancer Institute and an assistant professor of medicine at Harvard Medical School, both in Boston, Massachusetts.
Risk-Adapted Therapy for HPV-Positive Tumors
Several studies are assessing a reduced radiation dose for patients with HPV-positive head and neck cancer. The standard radiation dose for locoregionally advanced head and neck cancer is 70 Gy, which Hanna mentioned is one of the highest in all of oncology, warranting deintensification to avoid morbidity. Across these studies, clinical characteristics are being used to further classify risk for those with HPV-positive disease, such as tumor size, margins following surgery, extracapsular spread (ECS), and lymph node involvement.
The phase 2 NRG-HN002 study (NCT02254278)4 specifically examined a 60-Gy intensity-modulated radiation therapy (IMRT) dose either alone or with cisplatin. The 2-year progression-free survival (PFS) rate for patients who received IMRT plus cisplatin was 90.5% (90% lower confidence bound [LCB], 86.6%; P = .04), which met the primary end point for the trial, compared with 87.6% (90% LCB, 83.3%; P = .23) with IMRT alone. The MD Anderson Dysphagia Inventory mean score for the combination was 85.3 at 1 year, representing a significant improvement, Hanna said.
The NRG-HN005 study (NCT03952585) is exploring other combinations for patients with HPV-positive oropharyngeal squamous cell carcinoma, including 60 Gy with cisplatin or nivolumab (Opdivo), a PD-1 inhibitor. This phase 2/3 study is recruiting participants.
Other combination partners have been tested with radiation therapy, with varying results for patients with HPV-positive head and neck cancer. In the De-ESCALaTE HPV study (NCT01874171), the combination of 70 Gy of IMRT plus cetuximab (Erbitux) was inferior to cisplatin plus 70 Gy.5 Although this study did not show a superior partner to traditional platinum chemotherapy, other studies looking at induction chemotherapy followed by concurrent chemotherapy with low-dose radiation did show promise.
In the ECOG-E1308 study (NCT01084083),6 patients with HPV-positive cancers who experienced a complete response to induction therapy with cisplatin, paclitaxel, and cetuximab received low-dose IMRT at 54 Gy in 27 fractions plus weekly cetuximab. The 2-year OS with this approach was 94% (95% CI, 82%-98%). Moreover, quality-of-life improvements were noted, with fewer swallowing issues and less nutrition impairment than expected, Hanna said.
A similar approach with nab-paclitaxel (Abraxane) incorporated into the induction phase along with carboplatin was explored in the phase 2 OPTIMA study (NCT02258659).7 In this study, response to induction and clinical risk were used to tailor subsequent therapy. Patients with a low risk received 50 Gy of radiation therapy alone, whereas participants with intermediate to high risk received standard-dosed chemoradiotherapy. Overall, findings showed that the 2-year OS rate was 100% among patients with low-risk disease and 97% for those with high-risk disease.7
The subsequent OPTIMA II study (NCT03107182) moved this induction regimen to the locoregional setting with the addition of nivolumab to nab-paclitaxel and carboplatin.8 Findings showed the 2-year OS with the triplet induction followed by 50 Gy of radiation or surgery was 96.0% in the low-risk group, defined as those with postinduction shrinkage of 50% or more. The 2-year OS was 91.9% for the low-risk/ lower-response and high-risk/high-response group and 100.0% for an all-others high-risk group, which both received standard chemoradiotherapy after triplet induction.
“The concept is that people are trying to use lower-dose IO [immuno-oncology], radiation, or chemotherapy up front to select a patient for less radiation in the back,” said Hanna.
As with every successful strategy, the goal is to move a novel regimen earlier in the treatment paradigm. In the E3311 study (NCT01898494), risk stratification was moved into the adjuvant setting by applying it directly following transoral resection for patients with HPV-positive tumors. In this study, participants with T1-T2 N0-N1 tumors with negative margins were eligible for observation following surgery, whereas those with higher-risk disease received riskadapted treatments.
In findings from E3311,9 the 2-year PFS was 96.9% (90% CI, 91.9%-100%) for patients in the low-risk observation group after primary transoral surgery. Those with intermediate-risk disease (clear/close margins, < 1 mm ECS, 2-4 metastatic nodes) after surgery received either 50 Gy in 25 fractions or 60 Gy in 30 fractions, with similar outcomes: 2-year PFS rates of 94.9% (90% CI, 91.3%-98.6%) and 96.0% (90% CI, 92.8%-99.3%), respectively. Patients with high-risk disease (positive margins, > 1 mm ECS, ≥ 5 metastatic lymph nodes) received 66-Gy/33-fraction radiotherapy with cisplatin and had a 2-year PFS of 90.7% (90% CI, 86.2%-95.4%).
“Promising strategies exist, but where do you start?” asked Hanna. “Everyone is doing their own thing: less radiation, minimizing chemotherapy, using immunotherapy, selecting based on surgery, plasma HPV DNA. Stratification is really going to rely on biomarker selection being integrated into decision-making.”
Role of PD-L1 Expression in Head and Neck Cancer
National Comprehensive Cancer Network guidelines for head and neck cancer place the ICIs nivolumab and pembrolizumab (Keytruda) as category 1 preferred options for patients with recurrent, unresectable, or metastatic head and neck squamous cell carcinoma (HNSCC).10 However, these guidelines also note that the role and definition of PD-L1 expression remain ambiguous, with only an association seen between positive expression and better outcomes.
“We all know that PD-L1 expression is important in management of the disease. It was originally established with just basic immunohistochemistry that some squamous cell carcinomas do express PD-L1. Now, we have a little bit more clarity on how to quantify this in head and neck cancer,” Ranee Mehra, MD, said during a presentation at the 40th Annual CFS® conference. Mehra is director of head and neck medical oncology and a professor of medicine at the University of Maryland Marlene and Stewart Greenebaum Comprehensive Cancer Center in Baltimore, Maryland.
Clinical trials exploring immunotherapies in head and neck cancer have used 2 different definitions for PD-L1 positivity. The first, tumor proportion score (TPS), uses the percentage of tumor cells with PD-L1 expression on the membrane. The other measure, combined positive score (CPS), is the amount of PD-L1 expressed on immune cells divided by the number of tumor cells, with the final number then multiplied by 100. In both cases, the scores range from 0 to 100 and a score of 1 or greater indicates the cell is PD-L1 positive.
“The TPS score is used primarily in non–small cell lung cancer,” noted Mehra. “In head and neck cancer, we use CPS.”
The optimal method for measuring PD-L1 expression in head and neck cancer was established early in the development of ICIs for these cancer types, Mehra said. She described findings from the phase 1B KEYNOTE-012 study (NCT01848834) of pembrolizumab monotherapy in separate cohorts of patients with advanced solid tumors, including patients with recurrent/ metastatic HNSCC (Table).11
Table. ORR by PD-L1 Expression Status in KEYNOTE-012 Participants With HNSCC11
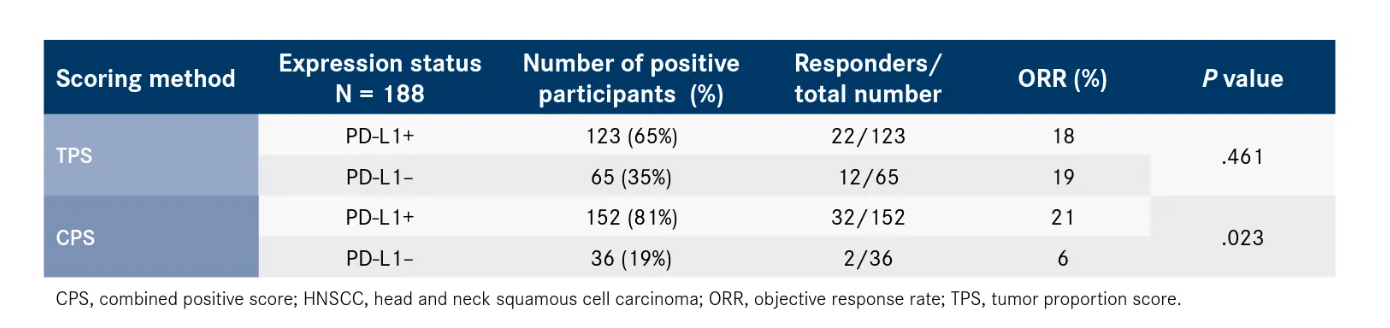
PD-L1 expression was examined by TPS and CPS in 188 patients with HNSCC. By the TPS measure, those with PD-L1–positive expression (n = 123) had an objective response rate (ORR) of 18% (95% CI, 12%-26%). Those whose tumors were PD-L1 negative by TPS (n = 65) had an ORR of 19% (95% CI, 10%-30%), providing little additional value for testing. By CPS, however, those with PD-L1–positive disease (n = 152) had an ORR of 21% (95% CI, 15%-28%), whereas those with PD-L1–negative expression (n = 36) had an ORR of 6% (95% CI, 1%-19%), suggesting a correlation with response.11
Although such findings are informative, responses to PD-1 inhibitors have been noted even in the absence of PD-L1 expression. Further, most studies have included patients with both positive and negative expression, with minor differences seen between the intention-to-treat (ITT) populations and PD-L1–based subsets in large phase 3 trials.
As an example, Mehra discussed the phase 3 KEYNOTE-048 study (NCT02358031), in which pembrolizumab was explored with or without the addition of platinum-based chemotherapy and 5-fluorouracil (5-FU) for patients with recurrent or metastatic head and neck cancer.
In 5-year findings from the study, which were presented at the European Society for Medical Oncology Congress 2022 in September (ESMO 2022),12 there was an improvement in OS seen with both pembrolizumab monotherapy and the combination of pembrolizumab and chemotherapy when compared with the EXTREME chemotherapy regimen alone, which comprises cetuximab, 5-FU, and platinum-based chemotherapy.
In the ITT population, the 5-year OS rate was 14.4% and 16.0% with pembrolizumab monotherapy and combination therapy, respectively, vs 6.5% and 5.2% with the EXTREME regimen.
In patients with a PD-L1 expression of 1 or more by CPS, the median OS with single-agent pembrolizumab was 12.3 months (95% CI, 10.814.8) compared with 10.4 months (95% CI, 9.0-11.7) for EXTREME (HR, 0.74; 95% CI, 0.610.89). Median OS was 13.6 months (95% CI, 10.7-15.5) for the combination of pembrolizumab and chemotherapy compared with 10.6 months (95% CI, 9.1-11.7) for EXTREME (HR, 0.65; 95% CI, 0.53-0.79). For those with a CPS of 20 or more, the benefit for the addition of the PD-1 inhibitor was more pronounced, with HRs of 0.61 (95% CI, 0.460.81) and 0.63 (95% CI, 0.47-0.84) for the single agent and combination vs EXTREME, respectively.
“Pembrolizumab was favored over EXTREME chemotherapy, in the intention-to-treat population and in the CPS greater than or equal to 1 population,” said Mehra. “It is gratifying to see survival data where we’re seeing survivals approaching 15% in 5 years for recurrent and metastatic head and neck cancer, which was previously unheard [of] in the era before immunotherapy.”
In a separate assessment of PD-L1 expression from KEYNOTE-048,13 patients with PD-L1 CPS expression of less than 1 had better outcomes with the EXTREME regimen compared with pembrolizumab. In those with PD-L1 CPS less than 1, the 12-month OS rate was 49% with EXTREME compared with 39% with single-agent pembrolizumab (HR, 1.51; 95% CI, 0.96-2.37; P = .96241). Moreover, in this same population, the 12-month OS was 47% with EXTREME compared with 41% with pembrolizumab plus chemotherapy (HR, 1.21; 95% CI, 0.761.94; P = .78932).
At PD-L1 CPS ranges of 1 to 19, the PD-1 inhibitor regimen began to emerge as a better option vs chemotherapy. For pembrolizumab monotherapy, the 12-month OS rate was 44% (95% CI, 35.1%-52.5%) vs 42.4% (95% CI, 33.9%-50.7%) with EXTREME, although this was not statistically significant (HR, 0.86; 95% CI, 0.66-1.12; P = .12827). For the combination of pembrolizumab plus chemotherapy, the 12-month OS rate was 52.6% (95% CI, 43.1%-61.2%) in those with a CPS of 1 to 19 vs 41.1% (95% CI, 32.4%-49.6%) with EXTREME (HR, 0.71; 95% CI, 0.540.94; P = .00726).13
“This was a subset analysis, and we still have the [ITT] population analysis, which showed the benefit of pembrolizumab monotherapy in PD-L1 expressers of greater than 1,” said Mehra. “I think there still is a role for using the KEYNOTE-048 regimens, but it is important to still utilize the CPS data to paint a full picture and to determine for an individual patient what type of regimen might be better.”
After showing initial success in the recurrent/metastatic setting, the investigation of pembrolizumab is beginning to move into earlier settings. For those with newly diagnosed locally advanced HNSCC, the KEYNOTE-412 study (NCT03040999) examined pembrolizumab with standard chemoradiation vs placebo plus chemoradiation, with findings presented at ESMO 2022.14
In the ITT population of KEYNOTE-412, the 36-month event-free survival (EFS) rate was 57.4% with pembrolizumab compared with 52.1% with chemoradiotherapy alone, which did not meet the threshold for statistical significance (HR, 0.83; 95% 0.68-1.03; P = .0429).
In subgroup analyses for EFS looking at PD-L1 expression by CPS, the HR was 1.09 (95% CI, 0.56-2.11) in patients whose tumors had a CPS of less than 1; however, it was 0.80 (95% CI, 0.641.00) favoring pembrolizumab with a CPS of 1 or more. In those with PD-L1 expression by CPS of 20 or more, the 36-month EFS was 66.7% with pembrolizumab/chemoradiation compared with 57.2% for chemoradiation alone; however, this did not reach statistical significance (HR, 0.73; 95% CI, 0.49-1.06).
The CPS subset analysis was more hypothesis generating, Mehra said. Moreover, she added that other studies have shown similar disappointing findings when combining immunotherapy with chemoradiotherapy, including those with the PD-L1 inhibitors avelumab (Bavencio) and durvalumab (Imfinzi).
“We have a few randomized trials now that are raising questions on how to incorporate immunotherapy with radiation,” she said. “Immunotherapy is not a radiation sensitizer. It does not have the DNA-damaging effects that cisplatin does. We have to stop thinking of it as a radiation sensitizer.”
Emerging Biomarkers and Imaging
In addition to HPV and PD-L1, indicators are emerging that could further risk-stratify therapy for patients with head and neck cancer. Epigenetic markers are under exploration, with some gene methylation patterns effectively predicting recurrence; however, these approaches are not ready for prime time, Hanna said.
A key imaging approach under exploration involves a tumor hypoxia assessment (FMISO). In the 30 ROC trial (NCT00606294) exploring this approach,15 tumors were resected and then a hypoxia assessment was completed using PET or CT scan and 18F-FMISO PET. Patients whose tumors were positive for hypoxia received standard 70-Gy radiotherapy plus cisplatin and those testing negative for hypoxia received 30 Gy of radiation plus cisplatin. This hypoxia measure was combined with HPV circulating plasma cell-free DNA (cfDNA) analysis to further predict risk.
Those in the low-risk group by cfDNA but with any type of clinical risk who had no hypoxia had a 2-year locoregional control rate of 94.4% (95% CI, 84.4%-100.0%) and a 2-year OS rate of 94.7% (95% CI, 85.2%-100.0%). Whole genome sequencing was also completed on the resected tumors, with detected DNA repair defects associated with response (P = .02).
“This is more than a 50% reduction in radiation,” said Hanna. “This is really exciting, and it is pushing the limits of how low you can really go with radiation doses.”
Another biomarker-based strategy on the horizon for risk-stratifying therapy involves the quantification of circulating tumor tissue-modified viral (TTMV) HPV DNA. When used as a method for posttreatment surveillance, TTMVHPV DNA had a positive predictive value of greater than 95% in a chart review involving data from 1076 patients.16 Additionally, the negative predictive value for TTMV-HPV DNA was also found to be 95%.
“HPV cancers have HPV virus in the tissue; it shouldn’t be anywhere else. If you have a tumor, and it sheds that virus at some rate, it is detectable in the blood. If I kill your cancer, I shouldn’t detect it in the blood,” Hanna said. “This is really transforming how we are thinking about HPV disease.”
Further work was completed to quantify the level of circulating tumor HPV DNA (ctHPVDNA), with the levels before and after treatment found to be informative of recurrence risk.17 Patients with a high baseline level of plasma ctHPV16DNA (> 200 copies/mL) that was reduced by 95% or more at day 28 post treatment with chemoradiation were found to have far superior outcomes, regardless of their clinical risk, compared with those with an unfavorable ctHPV16DNA clearance profile. Among patients with a favorable clearance profile, the regional disease-free survival (DFS) rate at 24 months was 100%. Those with poor clinical features and unfavorable ctHPV16DNA clearance had a 24-month DFS rate of 65%.
“I think the ctDNA is a great approach to get early signs of activity and response, especially for those more intermediate PD-L1 levels,” said Mehra. “I think incorporating imaging, how [patients are] tolerating treatment, and ctDNA are all great approaches.”
The TTMV-HPV DNA profile furthest along in development, known as NavDx, is being investigated as a means for risk-adapting therapy for patients with HPV-positive oropharyngeal cancer in the phase 2 ReACT study (NCT04900623). In ReACT , patients with intermediate clinical risk (T4, N0-2 and/or > 10 pack-year smoking history) will be stratified based on their ctHPVDNA clearance status following surgery. Those with a favorable risk by TTMV-HPV DNA clearance will receive a reduced dose of IMRT with or without low-dose cisplatin; those with unfavorable risk by ctHPVDNA will receive standard IMRT at 70 Gy plus cisplatin. The trial is recruiting participants.
There are various potential uses for a marker such as TTMV-HPV DNA, noted Hanna. “I actually use HPV DNA as a mechanism to monitor HPV-positive metastatic patients,” he said. “If they clear their DNA or I see the values are decreasing, I will feel more comfortable with an abbreviated PD-1 time course.”
Novel Therapeutics on the Horizon
The next step for personalized head and neck cancer treatment relies on a combination of strategies, Mehra noted. Several agents in the pipeline specifically target HPV, with the most promising being PDS0101, a T-cell–activating therapy specific to HPV, and CUE-101, a fusion protein designed to selectively deliver IL-2 to HPV-specific T cells.
Findings for both agents were presented at the 2022 American Society of Clinical Oncology Annual Meeting in June.18,19 For PDS0101 combined with pembrolizumab, the ORR was 41.2% in 17 patients with HPV-positive recurrent or metastatic HNSCC in the phase 2 VERSATILE-002 study (NCT04260126). The disease control rate with the combination was 76.5%. For CUE-101 plus pembrolizumab, the ORR was 28.6% among 7 evaluable patients with a disease control rate of 57.1% in a first-in-human study (NCT03978689). Both agents have received fast track designations from the FDA for head and neck cancer in combination with pembrolizumab. The designation for CUE-101 also covers its use as monotherapy.20,21
“These are things to watch for in the future, as ways to enhance immunotherapy response, at least for HPV-positive disease,” said Mehra.
References
1. Lewis A, Kang R, Levine A, Maghami E. The new face of head and neck cancer: the HPV epidemic. Oncology(Williston Park). 2015;29(9):616-626.
2. Cline BJ, Simpson MC, Gropler M, et al. Change in age at diagnosis of oropharyngeal cancer in the United States, 1975–2016. Cancers (Basel). 2020;12(11):3191. doi:10.3390/cancers12113191
3. Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363(1):24-35.doi:10.1056/NEJMoa0912217
4. Yom SS, Torres-Saavedra P, Caudell JJ, et al. Reduced-dose radiation therapy for HPV-associated oropharyngeal carcinoma (NRG Oncology HN002). J Clin Oncol. 2021;39(9):956-965.doi:10.1200/JCO.20.03128
5. Mehanna H, Robinson M, Hartley A, et al; De-ESCALaTE HPV Trial Group. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE HPV): an open-label randomised controlled phase 3 trial. Lancet. 2019;393(10166):51-60.doi:10.1016/S0140-6736(18)32752-1
6. Marur S, Li S, Cmelak AJ, et al. E1308: Phase II trial of induction chemotherapy followed by reduced-dose radiation and weekly cetuximab in patients with HPV-associated resectable squamous cell carcinoma of the oropharynx—ECOG-ACRIN Cancer Research Group. J Clin Oncol. 2017;35(5):490-497.doi:10.1200/JCO.2016.68.3300
7. Seiwert TY, Foster CC, Blair EA, et al. OPTIMA: a phase II dose and volume de-escalation trial for human papillomavirus-positive oropharyngeal cancer. Ann Oncol. 2019;30(2):297-302.doi:10.1093/annonc/mdy522
8. Rosenberg A, Agrawal N, Pearson AT, et al. Nivolumab, nabpaclitaxel, and carboplatin followed by risk/response adaptive de-escalated locoregional therapy for HPV-associated oropharyngeal cancer: OPTIMA II trial. J Clin Oncol. 2021;39(suppl 15):6011.doi:10.1200/JCO.2021.39.15_suppl.6011
9. Ferris RL, Flamand Y, Weinstein GS, et al. Phase II randomized trial of transoral surgery and low-dose intensity modulated radiation therapy in resectable p16+ locally advanced oropharynx cancer: an ECOG-ACRIN Cancer Research Group trial (E3311). J Clin Oncol. 2022;40(2):138-149.doi:10.1200/JCO.21.01752
10. NCCN. Clinical Practice Guidelines in Oncology. Head and neck cancers, version 2.2022. Accessed November 14, 2022. https://bit.ly/3E9l1kO
11. Mehra R, Seiwert TY, Gupta S, et al. Efficacy and safety of pembrolizumab in recurrent/metastatic head and neck squamous cell carcinoma: pooled analyses after long-term follow-up in KEYNOTE-012. Br J Cancer. 2018;119(2):153-159.doi:10.1038/s41416-018-0131-9
12. Tahara M, Greil R, Rischin D, et al. Pembrolizumab with or without chemotherapy for first-line treatment of recurrent/metastatic (R/M) head and neck squamous cell carcinoma (HNSCC): 5-year results from KEYNOTE-048. Ann Oncol. 2022;33(suppl7):S295-S322.doi:10.1016/annonc/annonc1056
13. Burtness B, Rischin D, Greil R, et al. Pembrolizumab alone or with chemotherapy for recurrent/metastatic head and neck squamous cell carcinoma in KEYNOTE-048: subgroup analysis by programmed death ligand-1 combined positive score. J Clin Oncol. 2022;40(21):2321-2332.doi:10.1200/JCO.21.02198
14. Machiels JP, Tao Y, Burtness B, et al. Primary results of the phase III KEYNOTE-412 study: pembrolizumab (pembro) with chemoradiation therapy (CRT) vs placebo plus CRT for locally advanced (LA) head and neck squamous cell carcinoma (HNSCC). Ann Oncol. 2022;33(suppl7):S808-S869.doi:10.1016/annonc/annonc1089
15. Riaz N, Sherman E, Pei X, et al. Precision radiotherapy: reduction in radiation for oropharyngeal cancer in the 30 ROC trial. J Natl Cancer Inst. 2021;113(6):742-751.doi:10.1093/jnci/djaa184
16. Berger BM, Hanna GJ, Posner MR, et al. Detection of occult recurrence using circulating tumor tissue modified viral HPV DNA among patients treated for HPV-driven oropharyngeal carcinoma. Clin Cancer Res. 2022;28(19):4292-4301.
doi:10.1158/1078-0432.CCR-22-0562
17. Chera BS, Kumar S, Beaty BT, et al. Rapid clearance profile of plasma circulating tumor HPV type 16 DNA during chemoradiotherapy correlates with disease control in HPV-associated oropharyngeal cancer. Clin Cancer Res. 2019;25(15):4682-4690.doi:10.1158/1078-0432.CCR-19-0211
18. Weiss J, Chintakuntlawar AV, Price KAR, et al. PDS0101, a novel type I interferon and CD8 T-cell activating immunotherapy, in combination with pembrolizumab in subjects with recurrent/metastatic HPV16-positive head and neck squamous cell carcinoma (HNSCC). J Clin Oncol. 2022;40(suppl 16):6041.doi:10.1200/JCO.2022.40.16_suppl.6041
19. Chung CH, Colevas AD, Adkins D, et al. Aphase 1 dose-escalation and expansion study of CUE-101, a novel HPV16 E7-pHLA-IL2-Fc fusion protein, given alone and in combination with pembrolizumab in patients with recurrent/metastatic HPV16+ head and neck cancer. J Clin Oncol. 2022;40(suppl 16):6045.doi:10.1200/JCO.2022.40.16_suppl.6045
20. PDS Biotechnology granted FDA fast track designation for lead candidate PDS0101. News release. PDS Biotechnology Corporation. June 2, 2022. Accessed November 15, 2022. https://bit.ly/39beCu4
21. Cue Biopharma granted FDA fast track designation for CUE-101 for the treatment of recurrent/metastatic head and neck squamous cell carcinoma. News release. Cue Biopharma. October 4, 2022. Accessed November 15, 2022. https://bit.ly/3SCsChQ
Leave A Comment
You must be logged in to post a comment.