Source: health.usnews.com
Author: Lisa Esposito, Staff Writer
Nearyly 450,000 Americans with swallowing or digestive problems manage tube feedings – also called home enteral nutrition – on their own. Some have temporary feeding tubes, while others leave the hospital with feeding tubes surgically placed for the foreseeable future.
Veteran users or “tubies” accept long-term feeding tubes as the best or only way to nourish themselves. Many resume school, work and social lives that were once threatened by severe weight loss and malnutrition. For them, getting a feeding tube means getting their active lives back.
Feeding Tube Benefits
Feeding tubes can prevent weight loss, boost energy and bolster your immune system. They also offer important health benefits for people coping with the following health issues:
Tube feeding for chronic swallowing challenges. For people with chronic health conditions that can cause swallowing difficulties, it helps keep them well-nourished. Neurologic conditions such as Parkinson’s disease, stroke or amyotrophic lateral sclerosis (ALS or Lou Gehrig’s disease) can impair nerves, affecting swallowing ability.
Tube feeding for oral and throat cancer. Inability to swallow food because of cancer of the mouth or throat is a major contributor to people receiving one, says Lisa Epp, a registered dietitian nutritionist with Mayo Clinic in Rochester, Minnesota.
Tube feeding for nutrition during recovery. A patient who has a short-term eating problem likely to eventually resolve, such as someone recovering from a surgery, brain injury or stroke, may benefit from having one.
Tube feeding for gastric problems. Gastric problems in which the stomach doesn’t empty well or a part of the intestine doesn’t work are the third major cause for feeding tubes, Epp says. Less commonly, trauma and paralysis impair the ability to swallow.
Tube feeding for kids with impaired eating ability. In kids, genetic and other disorders that affect their development can compromise their ability to swallow and eat. Premature infants, toddlers diagnosed with failure to thrive and kids with congenital heart defects, cerebral palsy, cystic fibrosis, GI tract malformations or gastroesophageal reflux disease (GERD) may be candidates for feeding tubes.
When children are barely able to eat because of chronic illness, feeding tubes must be considered, Epp says. If children can’t have needed surgery or chemotherapy because their bodies are weakened by malnutrition, parents have to make that difficult choice.
“Getting better nutrition is going to help them be stronger, increase their immune system and help children grow to their potential, whatever that potential can be,” Epp says. As for adult patients, she adds, “The No. 1 thing I hear when people come back at six-week and three-month visits is, ‘Why didn’t I do this sooner?'”
Maintaining a healthy body weight while tube feeding. Even though they can eat a certain amount of food, some people with gastric conditions can’t take in enough to maintain their health.
“An important consideration is if a patient is continuing to lose weight,” says Arlene Escuro, a dietitian and nutrition therapy specialist at the Center for Human Nutrition in the Digestive Disease and Surgery Institute at Cleveland Clinic. “The key is if they have a functional GI tract. We do have patients with a GI dysfunction (who are) able to take some food by mouth, but it’s not sufficient to sustain their nutrition, so they will need to continue on with the home tube-feeding regimen.”
Types of feeding tubes
Feeding tubes can be temporary or longstanding. Nasal tubes and gastric tubes are the two main types.
A nasal tube, which is usually temporary, is nonsurgical. Nasogastric tubes enter the body through one nostril and run down into the stomach. Another nasal tube, called a nasoduodenal tube, goes into the small intestine, or duodenum. A nasojejunal feeding tube goes into a farther part of the small intestine, the jejunum.
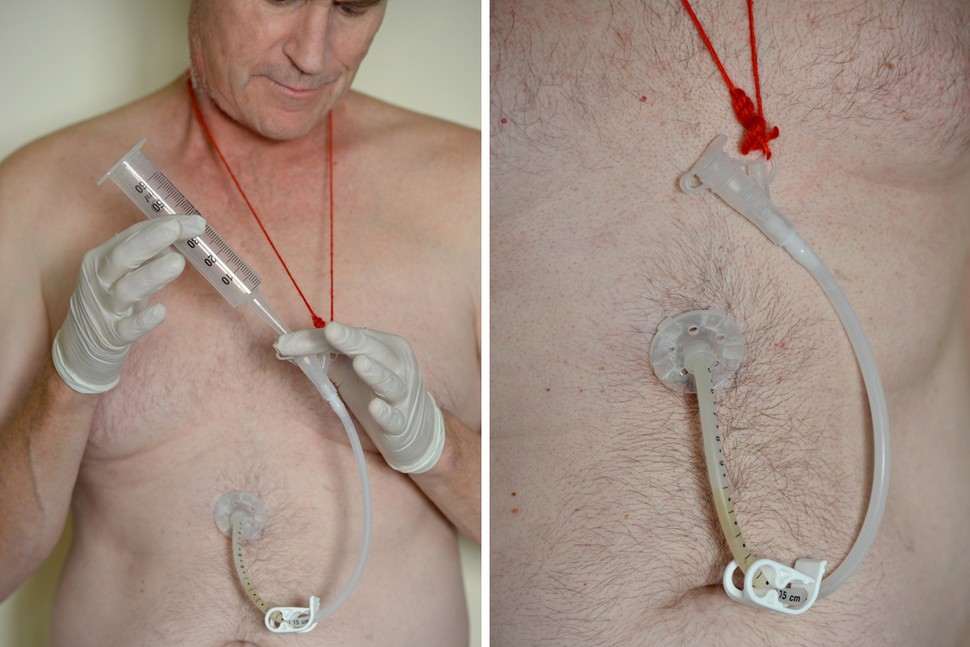
A gastrostomy tube, or G-tube, is often the choice for people who need longer-term feeding tubes. Surgeons use an endoscope to place the G-tube directly into the stomach. The surgery creates a stoma, a visible opening that connects to the feeding tube outside the body. The feeding tube allows people to take specialized liquid nutrition directly into their stomach.
Gastrostomy tubes are often referred to simply as PEGs. Specifically, PEG means percutaneous endoscopic gastrostomy. The visible portion of the feeding tube is permanently attached. However, people can transition to other options.
With buttons or low-profile feeding tubes, there’s no long outer tube attached to the stomach. Instead, users attach extension sets only when needed for feedings, water or medication. The button closure lies nearly flat against the stomach.
However, buttons aren’t the best option for everyone, Epp says. For instance, people who stay on a pump with continuous feeding throughout the day often prefer a tube, which can feel more secure.
Patients and families need to be fully informed of risks as well as benefits before a feeding tube is placed. Doctors evaluate a patient’s medical history to assess his or her individual risk and determine if there are any contraindications, or reasons against, having this procedure.
A variety of intestinal and esophageal conditions, a history of gastric bleeding, previous abdominal surgery and intractable diabetes are among the possible contraindications for G-tube feedings, according to comprehensive, evidence-based guidelines developed by the Cystic Fibrosis Foundation.
Mechanical risks involve tube malfunctions. For example, the tube can get blocked so feeding can’t get through, or it may become dislodged or fall out. It must then be replaced in a hospital.
Skin problems include redness and irritation around a patient’s stoma because of moisture build-up from the stomach or feeding leakage. “There’s also a risk of infection through the stoma site where (users) had a gastrostomy tube, a PEG tube, placed,” Escuro says.
Gastric side effects can develop as well. “GI complications could be diarrhea, constipation or under-hydration,” Escuro says. “Our goal when we have these patients, as we transition them from hospital to home, is to prevent readmissions and tube-feeding related complications.”
Tube Feeding Schedules
Feeding schedules range from episodic feedings at standard mealtimes to continuous feeding regimens.
“We make the regimen very individualized, as much as possible, so it will not interfere with patients’ lives,” Escuro says. Bolus or syringe feedings are larger feedings spread throughout the day like regular meals. It takes about 15 to 20 minutes to administer the formula, Escuro says, usually taken three to four times a day. “Basically, it’s like eating breakfast, lunch, dinner and a snack.”
Other patients go home with a pump for 24-hour feedings. “The reason for the pump feeding is that the feeding tube is placed in their small bowel,” Escuro says. “We don’t really recommend doing bolus feedings in the small intestine, just because it’s such a small reservoir, where most people will not tolerate bolus feedings.”
Pump feedings can be gradually spaced out for some people. “If they go home on continuous feeding when they’re hooked up to a feeding pump, we try to cycle their feedings, eventually.” Escuro says. “So from 24 hours we will gradually cycle them to 20 hours to 18, 16 and to 12 hours or so. If it’s in the stomach, we can transition a patient to bolus feedings.”
Eventually, some patients are weaned off feeding tubes altogether.
Managing a Feeding Tube
Learning how to manage and become comfortable with home tube feeding ideally starts before patients leave the hospital.
At Cleveland Clinic, patients and family caregivers start home enteral feeding education, which includes hands-on practice, before discharge. After discharge, Escuro says, patients with PEGs receive care from a home health nurse to check the stoma site and make sure it’s healing properly. In addition, a home care dietitian follows up to make sure patients are doing well.
Still, for a patient coming home with a tube placed in his or her stomach, the responsibility can seem overwhelming. Through practice, they master the following steps to successfully manage the feeding tube:
- Prepare the tube feeding
- Gather supplies
- Position for feeding
- Check residual contents
- Run continuous/cyclic tube feeding
- Infuse a bolus tube feeding
- Clean skin around tube site
- Clean tube feeding equipment
- Troubleshoot or report problems
Not Best for Everyone
A feeding tube is not always the right choice. For example, people with severe Alzheimer’s disease in later stages often have trouble eating and drinking. However, a feeding tube might not be for the best, according to Choosing Wisely, an initiative focused on avoiding unnecessary medical tests, treatments and procedures.
A frail older adult with Alzheimer’s could be at greater risk of complications such as pneumonia or pressure sores on the skin. They may lose the human contact of being fed by hand as well as the sensation of tasting food.
“Don’t recommend percutaneous feeding tubes (PEGs) in patients with advanced dementia – instead, offer oral assisted feeding,” tops a list of recommendations for physicians regarding quality of life for older adults from the American Geriatrics Society.
<u>Feeding Tube Food</u>
Commercial tube-feeding formulas are available to meet users’ individual nutritional needs. However, just as consumers of traditional food want more natural, less-processed options including plenty of fruits and vegetables, a similar movement is afoot among feeding tube users.
Blenderized whole foods, either made at home or commercially, are choices for patients who feel they can tolerate them better or who simply want to eat what others do. “It’s basically joining the family during mealtime and getting the same food, but it’s just blenderized,” Escuro says.
Expense is an issue. Users must work with insurers to cover ongoing costs of feeding supplies, particularly the food itself. While insurance usually covers the surgical placement, people pay at least a portion for tube-feeding formulas out of pocket.
<u>Resources for People With Feeding Tubes</u>
In addition to turning to their health care teams, people on home enteral nutritional can go online for expertise, advice and peer support.
The Feeding Tube Awareness Foundation is a nonprofit group whose mission is to support parents of children who are tube-fed.
Leave A Comment
You must be logged in to post a comment.