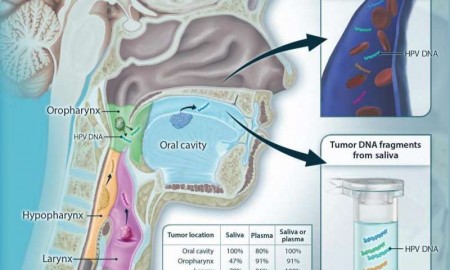
Schematic showing the shedding of tumor DNA from head and neck cancers into the saliva or plasma. Tumors from various anatomic locations shed DNA fragments containing tumor-specific mutations and human papillomavirus DNA into the saliva or the circulation. The detectability of tumor DNA in the saliva varied with anatomic location of the tumor, with the highest sensitivity for oral cavity cancers. The detectability in plasma varied much less in regard to the tumor’s anatomic location. Credit: Wang et al., Science Translational Medicine (2015)
On the hunt for better cancer screening tests, Johns Hopkins scientists led a proof of principle study that successfully identified tumor DNA shed into the blood and saliva of 93 patients with head and neck cancer. A report on the findings is published in the June 24 issue of Science Translational Medicine.
“We have shown that tumor DNA in the blood or saliva can successfully be measured for these cancers,” says Nishant Agrawal, M.D., associate professor of otolaryngology—head and neck surgery—and of oncology at the Johns Hopkins University School of Medicine. “In our study, testing saliva seemed to be the best way to detect cancers in the oral cavity, and blood tests appeared to find more cancers in the larynx, hypopharynx and oropharynx. However, combining blood and saliva tests may offer the best chance of finding cancer in any of those regions.”
Agrawal explains that inborn genetic predispositions for most head and neck cancers are rare, but other mutations that don’t generally occur in normal cells have long been considered good targets for screening tests.
In the case of head and neck cancers associated with HPV—tumors on the rise among Americans—Agrawal and his colleagues searched patients’ blood and saliva samples for certain tumor-promoting, HPV-related DNA. For non-HPV-related cancers, which account for the worldwide majority of head and neck tumors, they looked for mutations in cancer-related genes that included TP53, PIK3CA, CDKN2A, FBXW7, HRAS and NRAS.
The major risk factors for head and neck cancers are alcohol, tobacco—including chewing tobacco—and HPV infection.
For the study, 93 patients with newly diagnosed and recurrent head and neck cancer gave saliva samples, and 47 of them also donated blood samples before their treatment at The Johns Hopkins Hospital and MD Anderson Cancer Center in Texas. The scientists detected tumor DNA in the saliva of 71 of the 93 patients (76 percent) and in the blood of 41 of the 47 (87 percent). In the 47 who gave blood and saliva samples, scientists were able to detect tumor DNA in at least one of the body fluids in 45 of them (96 percent).
When the scientists analyzed how well their tumor DNA tests found cancers in certain regions of the head and neck, they found that saliva tests fared better than blood tests for oral cavity cancers. All 46 oral cavity cancers were correctly identified through saliva tests, compared with 16 of 34 oropharynx cancers (47 percent), seven of 10 larynx cancers (70 percent) and two of three hypopharynx cancers (67 percent).
The oral cavity refers to areas within the mouth, including the lips, front of the tongue, cheeks and gums. The oropharynx and hypopharynx are located in the back of the throat. The larynx, also in the throat, is typically known as the voice box.
“One reason that saliva tests may not have been as effective for cancer sites in the back of the throat is because we didn’t ask patients to gargle; we only asked them to rinse their mouths to provide the samples,” says Agrawal, a member of Johns Hopkins’ Kimmel Cancer Center and Ludwig Center.
Blood tests correctly identified tumor DNA more often in 20 of 22 oropharynx cancers (91 percent), six of seven larynx cancers (86 percent) and all three hypopharynx cancers. Taken together, blood and saliva tests correctly identified all oral cavity, larynx and hypopharynx cancers and 20 of 22 oropharynx cancers (91 percent).
Agrawal says the sensitivity of the tests overall depended on the cancer site, stage and HPV status, ranging between 86 to 100 percent. He also reports that saliva tests performed better for early-stage cancers, finding all 20 cancers, compared with blood tests that correctly identified seven of 10. He and his team found the opposite was true for late-stage cancers: Blood tests found more late-stage cancers (34 of 37), compared with saliva tests (51 of 73). Blood tests also correctly identified HPV-related tumors, occurring in 30 of the 93 patients, more often than saliva tests, probably because HPV-related tumors tend to occur in the back of the throat, which may not have been reached with the saliva rinse.
“Our ultimate goal is to develop better screening tests to find head and neck cancers among the general population and improve how we monitor patients with cancer for recurrence of their disease,” says Bert Vogelstein, M.D., the Clayton Professor of Oncology at the Johns Hopkins Kimmel Cancer Center, co-director of the Ludwig Center at Johns Hopkins and a co-author of the study.
The scientists caution that further study of their tumor DNA detection method in larger groups of patients and healthy people is needed before clinical effectiveness can be determined, and that refinements also may be needed in methods of collecting saliva and the range of cancer-specific genes in the gene test panel.
In addition, Agrawal says: “We don’t yet have definitive data on false positive rates, and won’t until there are more studies of the tests in healthy people.” However, he notes, the formulas used to analyze their blood and saliva tests are designed to weed out questionable results.
False results in gene tests arise when DNA are copied many times, sequenced and analyzed. The scientists used a method they developed and tested previously in cervical fluid to find ovarian and cervical cancers. Specifically, they attach a kind of genetic bar code—a random set of 14 DNA base pairs—to trace each copied DNA fragment to its original one. DNA copies lacking the bar code are suspected to be an artifact of the process, and any mutation found in it is disregarded.
Agrawal says that tests like the one his team used, if used commercially, likely would cost several hundred dollars, and “our long-term goal is to create a test that costs less than $50 so it can be administered by physicians or dentists.”
To screen for head and neck cancers, which occur in more than 50,000 people in the U.S. each year, doctors conduct physical examinations. Biopsies are taken of suspicious-looking lesions, but “this method is not ideal, as evidenced by the fact that most head and neck cancers are rarely found at very early stages, when they are most curable,” says Agrawal.
*This news story was resourced by the Oral Cancer Foundation, and vetted for appropriateness and accuracy.
Leave A Comment
You must be logged in to post a comment.